Published: 01/2024
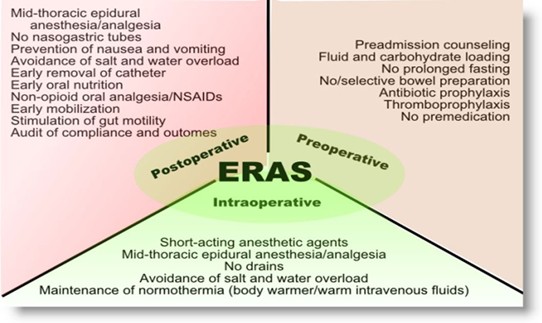
Enhanced recovery after surgery (ERAS) protocols aim to maintain normal physiology for surgical patients and are widely credited with improving historic practices such as prolonged fasting for preoperative patients. Evidence-based medicine drives ERAS care protocols across the range of surgical specialties. Common principles are summarized in Figure 1. In specialties such as colorectal surgery and GYN Oncology, ERAS protocols have been shown to decrease hospital length of stay, reduce opioid utilization and readmissions, and improve patient satisfaction.
Common characteristics of pre-operative protocols for gynecologic and gynecologic oncology surgery involve optimizing nutrition for patients prior to surgery by drinking a clear carbohydrate beverage two hours prior to procedures to reduce the negative effects of fasting. Infection prevention recommendations include showering with chlorhexidine soaps, trimming (not shaving) body hair, and judicious use of bowel preparation. Patient counseling is also critical regarding expectation setting for hospital length of stay and ambulation timeline.
Immediately prior to surgery, a typical protocol will recommend administering medications to reduce need for opiate analgesia. Acetaminophen, gabapentin, and celecoxib are commonly administered in the pre-operative area. Thromboprophylaxis with sequential compression devices and/or subcutaneous anticoagulants (such as heparin) are often indicated. Vaginal preparation with povidone-iodine should be considered prior to cesarean delivery.
Intraoperatively, checklists are utilized to confirm antibiotics were given prior to procedure start and are repeated for excessive blood loss or prolonged surgery length. Euvolemia with judicious crystalloid intravenous fluid administration and patient normothermia are emphasized. For high-risk patients, nausea prevention with dexamethasone and scopolamine patches at the time of induction is recommended. Opioid requirements can be minimized with techniques such as epidural regional anesthesia and intraoperative transabdominal plane (TAP) blocks, in addition to avoidance of painful stimuli such as abdominal drains and vaginal packing. ERAS protocols should also be implemented in Obstetrics to support “the evidence-based Cesarean” with guidance provided on techniques such as uterine and skin closure techniques.
Features of post-operative ERAS protocols highlight the need for early ambulation and early feeding. Scheduled NSAIDS and acetaminophen are recommended. Patient-centric narcotic administration such as a PCA (Patient Controlled Anesthesia) can be utilized. Post-operative anticoagulation is recommended in high-risk patients.
Specific protocols and dosages vary depending by institution. When implementing ERAS protocols, collaborate with informatics to create easily accessible order sets or bundles for the electronic medical record. Evaluate outcome measures, including patient length of stay, total cost, and total number of pills of opioids prescribed at discharge. Patient satisfaction with preoperative counseling and provider adherence to utilizing the order sets and each step in the protocol are process metrics to consider. Ongoing cyclic improvement efforts will likely be necessary to reach targets as ERAS is a major culture change.
Example: Dr. X has been practicing at University Hospital for 40 years as a GYN oncologist. They routinely order a mechanical bowel prep for all patients undergoing cytoreductive debulking. While reviewing process measure data, the multidisciplinary team becomes aware that Dr. X has not yet begun ordering antibiotics with their bowel preps. The department’s quality champion sits down with Dr. X to review strong evidence showing mechanical bowel prep alone actually increases infectious complications such as anastomotic leak. Dr. X is excited to incorporate this evidence into their practice and begins utilizing mechanical bowel prep with oral antibiotics the day prior to surgery.
Figure 1. Visual representation of common ERAS principles for perioperative care.
https://www.anesthesiallc.com/publications/blog/entry/enhanced-recovery-after-surgery-andanesthesia
Additional Reading
Perioperative pathways: Enhanced recovery after surgery. Committee opinion, ACOG. Number 750 (Reaffirmed 2020). Committee on Gynecologic Practice.
Caughey A, et al. Guidelines for intraoperative care in cesarean delivery: Enhanced Recovery After Surgery Society Recommendations (Part 2). American Journal of Obstetrics and Gynecology Volume 219, Issue 6, December 2018, 533-544.